There’s a virus you may have never heard of before that is estimated to infect up to 90 percent of people and lurks quietly in your cells for life—but if it becomes activated, it will destroy your brain. If that’s not startling enough, researchers reported this week that there may be a new way for this virus to activate—one that affects up to 10 percent of adults worldwide.
The virus is the human polyomavirus 2, commonly called either the JC virus or John Cunningham virus, named after the poor patient from whom it was first isolated in 1971. It shows up in the urine and stool of infected people and spreads via the fecal-oral route. Many people are thought to be infected early in life, and blood testing surveys have suggested that 50–90 percent of adults have been exposed at some point.
Researchers hypothesize that the initial site of infection is the tonsils, or perhaps the gastrointestinal tract. But wherever it happens, that initial infection is asymptomatic. At that point, a person is infected with what’s called the archetype JC virus, which quietly sets up a persistent but utterly silent lifelong infection.
For the vast majority of people, that is all their JC virus infection will be—silent. But for an unlucky few, the JC virus will seemingly awaken, rearrange its genetic material, and morph into a brain-demolishing nightmare that causes a disease called progressive multifocal leukoencephalopathy or PML.
Devastating disease
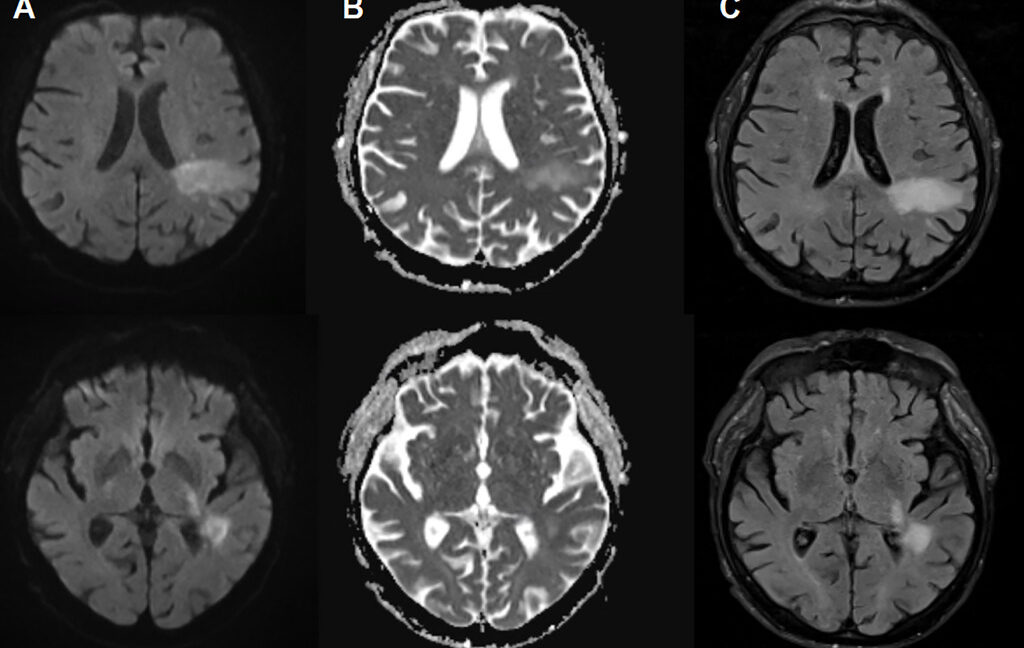
In PML, the new disease-causing virus or “PML-type” JC virus actively invades the brain, blowing up specific brain cells, including the cells that form the insulating myelin sheaths that protect nerve cells. This leads to extensive demyelination, which results in nerve cell dysfunction and death. On imaging, PML can show up as signature lesions in the brain. Those imaged lesions, paired with test findings of JC virus DNA in cerebrospinal fluid, are how PML is diagnosed. But for patients experiencing PML, the symptoms can mimic everything from a stroke to multiple sclerosis, causing problems like speech impairments, visual defects, motor dysfunction, and seizures.
PML was first identified in 1958 in a cancer patient. But it was considered an extremely rare condition until the 1980s, when it started to be seen in patients with HIV/AIDS. In fact, PML became an AIDS-defining disease, with 2–5 percent of HIV-infected patients developing it in the early phase of the epidemic. At that point, the condition was uniformly fatal. But with the introduction of highly active antiretroviral therapy (HAART) in 1996, PML cases declined, and the disease was no longer a death sentence, though survivors often have significant lasting damage.
Facts Only
The human polyomavirus 2, or JC virus, infects an estimated 50–90 percent of adults.
It was first isolated in 1971 from a patient named John Cunningham.
Transmission occurs via the fecal-oral route, with the virus detected in urine and stool.
Initial infection is asymptomatic and often occurs early in life.
The virus establishes a persistent, lifelong infection in most individuals.
In rare cases, the virus can mutate into a neurovirulent form, causing progressive multifocal leukoencephalopathy (PML).
PML destroys myelin-producing cells, leading to neurological symptoms such as speech impairments, visual defects, and seizures.
PML was first identified in 1958 and became more prevalent during the HIV/AIDS epidemic.
Before antiretroviral therapy (HAART), PML was uniformly fatal in HIV/AIDS patients.
HAART, introduced in 1996, reduced PML fatalities but often left survivors with significant neurological damage.
Recent research suggests a potential new activation pathway for the virus, affecting up to 10 percent of adults.
Executive Summary
Full Take
The narrative around the JC virus and PML is compelling because it taps into deep-seated fears of hidden, incurable threats—viruses lurking silently in our bodies, capable of sudden, catastrophic activation. The strongest version of this story highlights legitimate scientific concerns: a ubiquitous virus with a rare but devastating outcome, historically linked to immunocompromised populations, now potentially emerging in new contexts. The framing leans on the dramatic contrast between the virus’s ubiquity and its rarity in causing disease, which is factually accurate but also amplifies its perceived menace.
Pattern-wise, the piece employs a classic fear appeal (ARC-0012 Fear Exploitation) by emphasizing the virus’s near-universal presence and its brain-destroying potential, though it stops short of sensationalism. There’s no overt distortion, but the focus on the "brain-demolishing nightmare" risks overshadowing the statistical reality: PML remains exceedingly rare. The historical context—HIV/AIDS and PML’s shift from fatal to manageable—serves as a useful anchor, but the mention of a "new way for this virus to activate" lacks mechanistic detail, leaving room for speculative anxiety.
Root cause: The narrative reflects a broader paradigm of emerging infectious threats, where scientific uncertainty meets public health communication. The unstated assumption is that rare but severe outcomes warrant heightened attention, even when absolute risk remains low. This echoes historical patterns of disease framing, where conditions like PML gain prominence during epidemics (e.g., HIV/AIDS) but recede in public consciousness once treatments mitigate their impact.
Implications: For human agency, the story underscores the limits of individual control—most people harbor the virus, yet few can influence its reactivation. The costs are borne by the unlucky few who develop PML, while the benefits of awareness accrue to researchers and public health systems. Second-order consequences may include unnecessary anxiety among immunocompetent individuals or, conversely, complacency if the risk is perceived as too remote.
Bridge questions: How should public health messaging balance awareness of rare but severe risks without inducing disproportionate fear? What gaps exist in our understanding of JC virus reactivation, and how might they be filled? Would your perception of this threat change if the activation mechanism were better understood?
Counterstrike scan: A bad actor pushing this narrative might amplify the "brain-demolishing" angle while downplaying rarity, fostering panic. They could also exploit the HIV/AIDS historical link to stoke stigma or distrust in medical systems. However, the actual content avoids these tactics, presenting the science without undue alarmism. The piece is clean—no structural alignment with manipulation playbooks.
Sentinel — Likely Human
This report details the JC virus, a persistent infection found in most adults, which can sometimes trigger PML, a devastating brain disease. The analysis suggests a human-generated text due to its adherence to established reporting patterns and absence of stylistic anomalies.